Cervical Spine Myelopathy & Radiculopathy -

Вставка
- Опубліковано 8 жов 2023
- Cervical Spine Myelopathy & Radiculopathy
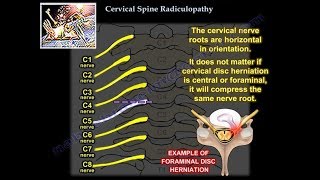
Cervical spine myelopathy can occur due to compression of the cervical spinal cord. Patient with cervical spine myelopathy will have gait disturbance. Gait disturbance is an indication for surgery. X-ray will show spondylosis and loss of lordosis. MRI will show compression of the cervical spinal cord. Some of these patients will have lumbar spinal stenosis, and they come to the doctor with an MRI, and they have gait disturbance. Check the cervical spine. Get an MRI of the cervical spine. The patient examination may be confusing, because they will come to the doctor with low back pain and a positive MRI for lumbar spinal stenosis. Ask about neck pain and stiffness, and also if the patient feels unstable when walking. Then examine the patient for upper motor neuron signs: spasticity, hyperreflexia, Hoffman’s sign, Clonus, or Babinski reflex. The presence of this reflex indicates an upper motor neuron lesion due to cervical spinal cord compression. Gait disturbances can also occur with thoracic disc problems, which occur more in males. There will be pain with radicular symptoms, with normal upper extremity exam, and there will be upper motor neuron findings in the lower extremity such as clonus and Babinski reflex. Usually you will do anterior approach of the cervical spine especially when there is a kyphotic spinal segment. Go anterior, especially if there is cervical spine kyphosis more than 10 degrees, because this can be corrected anteriorly. You may go posteriorly, (laminectomy and posterior fusion), but kyphosis more than 10 degrees is contraindication to going posteriorly. Usually this operation is done for multilevel decompression. Infection is a complication of the posterior approach. If you do laminectomy alone, you will have progressive kyphosis. C5 nerve root palsy may occur due to the anterior and posterior approach (unknown why it occurs, the nerve recovers but takes a long time to recover). The recurrent laryngeal nerve (RLN) can cause vocal cord paralysis on one side will give hoarseness. The superior laryngeal nerve (SLN) will affect the high note phonation, it can affect singers, there will be no vocal cord paralysis. This usually occurs when dealing with upper cervical spine surgical approaches. 50% of neck rotation is between C1 and C2. Flexion/extension mostly occurs at the level of C4-C5. Pain and/or neurological symptoms resulting from conditions such as a disc herniation that irritates a nerve in the cervical spine. Cervical spine and shoulder problems overlap. The patient’s symptoms are relieved by shoulder abduction and placing the hand over the head. In cervical disc problems, be aware of false positive MRIs. Cervical disc problems usually affect the lower nerve root. With compression of the C7 nerve root, there will be middle finger numbness, triceps weakness, and the triceps reflex will be affected. The cervical nerve roots are horizontal in orientation. It does not matter if cervical disc herniation is central or foraminal, it will compress the same nerve root. C7 nerve root runs above the pedicle of the C7 vertebra. The patient will come to the doctor with unilateral arm pain that is relieved by arm elevation. The numbness and paresthesia will occur in specific dermatomes. When you examine the patient, do provocative tests such as the Spurling’s test and the shoulder abduction test. Even if there is a bad cervical spine disc problem of MRI, treat it conservatively for about 3 months. Give the patient therapy and nonsteroidal anti-inflammatory drugs (NSAIDs). 75% of the patients will improve with nonoperative treatment. Do surgery when there is progressive pain for 6-12 weeks and progressive neurological deficit.








Thank you very much!
I am scheduled for my MRI next week and hope to finally get some visual answers. I am actually suffering from both!
I have gotten a better understanding of my injuries and been able to assist my Doctors more clearly with my diagnosis because of you and for that I am so grateful. 🙏❤
Excellent presentation with clear succinct explanations.
Thanks
شكرا لك
thanks
Thanks doctor
💝
Thank you so much.
You are so welcome
Hi I'm the absolute opposite, I've leg weakness and numbness from 6_6 c-7 herniation, my ulnar forearms are on fire, I've no power loss in arms or fingers but i have the little finger escape from left hand, mine was an impact from a fall, I've had discectomy done but I haven't recovered, pain in my legs is unbelievable while walking and I've no idea what to do!
sorry c-6 c-7 herniation
Shut
Make video on Hirayama disease
Thanks doctor
How can I meet you
THANKS