Love this video? Check out our ECG/EKG course made entirely with videos like this: Students, click here: www.alilaacademy.com/courses/ecg-ekg-for-students Teachers, click here: www.alilaacademy.com/courses/ecg-ekg-for-teachers
I know this video is several years old but this helped me understand what was happening to a pt today in the ED. I appreciate your videos are straightforward with easy-to-follow diagrams/visuals. Thank you for your work.
Thank you for this wonder animation explaining hyperkalemia. I was diagnosed with hyponatremia and seek to understand via an animation how low serum sodium (hypernatremia) impacts the body's electrolyte balance. An animation of the body's electrolyte balance including the sodium-potassium pump of the cell would be very helpful. It makes sense that too much water without salt can be very detrimental to the optimal function of the sodium-potassium cell. I would LOVE a series of animations to offer a comprehensive understanding of both hypernatremia and hyponatremia. PLUS, cause-effect symptoms and both clinical and alternative treatments.
Amazing wow totally makes sense and I cant believe that many people in the medical field doesn't even cross their mind orr had any idea that i could actually have this.. Thank you so much for the knowledge, keep up the great work and God bless you and yours.
I just had this it almost killed me when I went to the emergency room they gave me insulin a nebulizer and two IVs of fluid it worked in an hour I was out of there I thought they were going to have to keep me in the hospital but it was a quick treatment I quit taking potassium powder and just get what I need out of vegetables
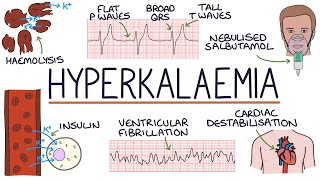
Excellent video that talks about the RMP being raised due to the inhibition of efflux of potassium out of the cell. One addition, the Ca++ is giving to stabilize the cardiac membrane potential; however, Ca*+ stabilizes the membrane potential by raising the threshold potential. The raise in threshold potential counteracts the raised RMP, enabling activation of sodium channels to maintain influx of sodium intracellularly . Furthermore, treatment of insulin, usually 10 units, helps drive glucose and potassium intracellularly. This can cause iatrogenic hypoglycemia. The provider should administer glucose to supplement the effect of possible hypoglycemia.
i would like to comment on what was said in the video, in 4:18 about treating it with Ca,, now Ca is called the bodyguard of Na channels, it dose so by slowing down the influx of Na,, thats because Ca ion has positive charge, also Na ion has +ve charge, so repulsion will occur between them thus slowing each other down :V now in mild hyper-kalemia as what said it causes hyper-activity in nerves, because it makes the cell more +ve ( so treating it with Ca (which slows down Na influx causing hypo-function) is all good but treating hyperkalemia with it is not, because as we said (8month ago xD (back then i remember i was in last week of Cardio module)) anyhow, hyperkalemia causes hypo-acitivty, because it make nerves sticks in absoulte-refractory peroid ("because Na inactivation gate still activated,,, and all that which i mentioned in the comment") anyhow, hyperkalemia causes hypo-acitivty and adding Ca will worsen it not fixing it as before,, thus Ca shouldnt be given
Wowww superb ,very short but very sweet lecture.it will help all medical professionals.thank you.if possible do a vedios of pottasium Vs sodium in body how it's co related. Also hyperkalemia Vs hypokalemia
I have been so freaking confused between Hyperkalemia and Hypokalemia and how they relate to Cardiac Arrest; correct me if I'm wrong, but I think it simplifies down to this: Hyperkalemia - the cell has difficulty contracting, Hypokalemia - the cell has difficulty relaxing
"There appears to be a direct effect of elevated potassium on some of the potassium channels that increases their activity and speeds membrane repolarisation." You're welcome :))
Threshold Potential does not move, but the RMP moves up closer to Threshold Potential if there is decrease in electric gradient: less K+ leaks from ICF to ECF, more K+ in ICF leads to decrease value (-90mV to -65mV) of RMP.
No it’s not about absolute values it’s about potential DIFFERENCE . RMP is the concentration gradient across the membrane. Suppose initially there were 100 k+ions inside and zero outside . The difference would be 100 making the rmp -100 mV . Now if 25 k+ ions move outside, only 75 remain inside making the difference 50 so rmp is now -50 mV which is closer to threshold potential. Hope this helps
What I don't understand is why hyperkalemia makes the membrane potential less negative? If you have more potassium ions in the extracellular fluid, doesn't that mean you have more positive charge outside? Wouldn't that make the membrane potential more negative?
i guess because -ve rmp is reached by efflux of k+ during repolariztion) (and this efflux depend on diffusion, its not active process, it depend on conc. gradient) now as K+ can't leave (or to be more correct, less K+ is leaving cell because of the changed k gradient) cell wont reach the normal negativity (RMP), it will be less negative, this will make cell more excitable (its closer to firing thresold, less stimuli is required to reach firing level and causesing A.P (All na channels to be open) but in severe hyperkalemia, a very little amount of K+ leave the cell, cell wont even reach the firing level, it will be higher than normal threshold level thus the inactivated sodium channel will stay in its inactivation state (inner inactivation gate still closed (remember that Na channels has 2 gates, one when activated causes depolarztion and other when activated close the channel and causes the absoulte r. peroid) ),, in other word, it will stay in absoulte refractoy peroid -> less excistability (or even NEVER exctitable) btw thats why K+ was used as execution injection, and thats why when K+ level reach 7mg/dl you should do dialysis right away, no time for insulin (althou the very rapid action of insulin)..
Let me try to make you understand Hyper kalemia means inc levels of potassium in the ecf as we knis that potassium is 20 times more in icf comparred to ecf so just as thete is mkre potassium outside the potassium inside shall also increase to maintain a conc diff resultantly tye inside will become less negative and the membrane potential will bexome less negative as well or one can say partial state of depolarization it will never reach the rmp of compltetw its re polarization
Maybe its because of that inside of the cell, amount of potassium isnt changing. Instead of that we take more potassium from the outside. In the end we had more possitive ions in the ecf comparing with the first situation. That can be cause of less negativity of the membran potential.
Its because high conc of potassium outside will decrease the conc gradient across the membrane.. So less potassium will move out the cell.. Making the inside more positive or less negative
The T waves show you the electrical signal when the cardiac myocytes are repolarizing. I know that you need the sodium/potassium pump to work to restore concentration gradients... maybe that's an easier job when you're not fighting as high a concentration gradient so it goes up more quickly? That's probably wrong, but that's how I remember it...
@@poljakovaandrea2223 you know when the gradient of an ion increases across membrane its tendency to move to side with lower conc. increases, so when overall potassium increases in serum more than normal of it would percolate in the cell making inside of membrane less negative. I hope it helps :)
Mam which is the first mineral and vitamin to be depleted in hair cells during stress causing sudden graying of hairs is it sodium chloride iron or copper.or calcium
I had this pt who skipped her dialysis and came to ER for chest pain, she was bradycardic, she went unresponsive, her lab Potassium was 8.0 prior to hemodialysis. I don’t know if she survive, she left the room intubated, they took her for emergency hemodialysis.
How membrane potential becomes less negative when there is still the same amount of Kalium inside the cell and also same amaunt of negative charge. Should Hypercalemia outsuide of the cell contribute to positivity outside and thus increase potential difference from -90mv to maybe -120 mv and lead to hyperpolarization ?
Focus on the natural K+ leak channels. Less K+ leaks when hyperK in ECF (electric gradient is lessen). More K+ is retained in ICF that will move the RMP up closer to the AP threshold. Conversely, if hypoK+ occurs in ECF.
I have a hypotetical question, if I persons has CKF and also COPD, would that further increase the levels of K+??? I mean, the kidneys can't remove K+, the lungs keep building up CO2 in the blood which would leade to imbalance in PH since the cells would start exchanging K+ outside the cell and taking H+ in as a compensatory mechanism to reach back the normal levels of PH and correct the acidosis. In short, respiratory acidosis could worsen the increase of extracelular K+??? And also suppose that the patient takes Inhibitors of ACE, wouldn't that further spike K+ and maybe become a life threatening critical point to the patient's heart??
Insulin moves K+ from outside the cells into cells, thus decreasing K+ OUTSIDE the cells. K+ outside the cells = K+ in the blood. It's the K+ in the blood that is important, not the total K+









Love this video? Check out our ECG/EKG course made entirely with videos like this:
Students, click here: www.alilaacademy.com/courses/ecg-ekg-for-students
Teachers, click here: www.alilaacademy.com/courses/ecg-ekg-for-teachers
Finally after so many days I got the explaination of ECG PATHOPHYSIOLOGY IN HYPERKALEMIA.TY GUYS
Aniket Nerlekar m
The first part of this video is the same as the "hypokalemia" video. If you have watched our hypokalemia video, you may want to skip to 1:19.
the best explanation of effects of Hyperkalemia ever
I know this video is several years old but this helped me understand what was happening to a pt today in the ED. I appreciate your videos are straightforward with easy-to-follow diagrams/visuals. Thank you for your work.
The best explanation I've found on youtube! Thank you ❤
In using insulin for the treatment of hyperkalemia, glucose must be added to prevent iatrogenic hypoglycemia.
This is fantastic expkaibation I never heard before, Keep it up
Love the visuals!
Best ever explanation for hyperkalemia
i think i understand this more! tysm as always☺️
Yes. The best channel I have found in explaining EP . BEST WORK !
Great to hear!
finally got a discernible explanation
it's happy ;earning when we understand things tysm for providing that :))
thank you so muc,perfect explanation,perfect sound,100/100 marks
Excellent explanation of sodium and potassium pump.
❤❤❤❤ thank you
Excellent video!
It took me SEVERAL attempts and i still don't nearly get the ekg graph but this is incredibly interesting and well explained
Thank you.. Finally I got the explanation im looking for
Good explanation ! Thanks !
The best explanation. thank
thanks for clearing the concept
Thank you for this wonder animation explaining hyperkalemia. I was diagnosed with hyponatremia and seek to understand via an animation how low serum sodium (hypernatremia) impacts the body's electrolyte balance. An animation of the body's electrolyte balance including the sodium-potassium pump of the cell would be very helpful. It makes sense that too much water without salt can be very detrimental to the optimal function of the sodium-potassium cell. I would LOVE a series of animations to offer a comprehensive understanding of both hypernatremia and hyponatremia. PLUS, cause-effect symptoms and both clinical and alternative treatments.
Those subjects are on our list of videos to make, likely soon. Take good care of yourself!
This video gave me such an epiphany bless the heck out of you
Simple. Fantastic!
Thank you!
Amazing wow totally makes sense and I cant believe that many people in the medical field doesn't even cross their mind orr had any idea that i could actually have this.. Thank you so much for the knowledge, keep up the great work and God bless you and yours.
Thank you for the nice and clear explanation
this was actually incredibly informative
Amazing explanation
Yes....it was....amazing video ma'am
well explained ! Thank You
I just had this it almost killed me when I went to the emergency room they gave me insulin a nebulizer and two IVs of fluid it worked in an hour I was out of there I thought they were going to have to keep me in the hospital but it was a quick treatment I quit taking potassium powder and just get what I need out of vegetables
Thanks a lot ❤
Thanks ☺️
Thank you so much!!!!
may i know more deeply about how calcium infusion can reverse conduction abnormalities?
thank you very much
Very claire vidio and well explained.
amazing as always good job
Great video for learnig. Thankyou
Excellent!!!!
Excellent thank you.
your videos are awesome . good job
Beautiful explanation, couldn’t have been better.
Great educational video
Thank you
The Juice U came for 2:28
excellent presentatoin show ECG LEADS
Please make videos on test and clinical examination for central nervous system disorders
Thanks it’s was really informative
And tell me why T wave rise please?
The EKG explanation was great thanks!!
videos on hyper and hypo sodium, magnesium and phosphorous would be good
excelllent presentation
good, thank you
Excellent video that talks about the RMP being raised due to the inhibition of efflux of potassium out of the cell. One addition, the Ca++ is giving to stabilize the cardiac membrane potential; however, Ca*+ stabilizes the membrane potential by raising the threshold potential. The raise in threshold potential counteracts the raised RMP, enabling activation of sodium channels to maintain influx of sodium intracellularly . Furthermore, treatment of insulin, usually 10 units, helps drive glucose and potassium intracellularly. This can cause iatrogenic hypoglycemia. The provider should administer glucose to supplement the effect of possible hypoglycemia.
Thx alot , finally undrrstood hyperkalemia effect on heart
good
thanks
Thankyou
i would like to comment on what was said in the video, in 4:18 about treating it with Ca,,
now Ca is called the bodyguard of Na channels, it dose so by slowing down the influx of Na,, thats because Ca ion has positive charge, also Na ion has +ve charge, so repulsion will occur between them thus slowing each other down :V
now in mild hyper-kalemia as what said it causes hyper-activity in nerves, because it makes the cell more +ve (
so treating it with Ca (which slows down Na influx causing hypo-function) is all good
but treating hyperkalemia with it is not, because as we said (8month ago xD (back then i remember i was in last week of Cardio module)) anyhow, hyperkalemia causes hypo-acitivty, because it make nerves sticks in absoulte-refractory peroid ("because Na inactivation gate still activated,,, and all that which i mentioned in the comment")
anyhow, hyperkalemia causes hypo-acitivty and adding Ca will worsen it not fixing it as before,, thus Ca shouldnt be given
i’m confused now
at what point?@@retaa9282
about why effect of ca on hyperkalemia especially on the na interaction active open gate
Thanks so much very well explained video.
Please make a new video explaining boost of insulin in pancreas medically & or by diet & excercise.
Thanks
this video saved my life. 4 years of nursing school and I still never understood it full till this day.
are you 11 years old?
@@gustavoo3886 why is it relevant?
@@gustavoo3886 😂😂😂
Tq
great explanation. can u pls do a video on acid base balance and renal system?
It's on our list!
Thnx for great knowledge
Great video but no mention in the use of salbutamol as a treatment for hyperkalaemia?
thank you!!!!
thank you so much for 3:10, nobody could explain it to me properly >.
Wowww superb ,very short but very sweet lecture.it will help all medical professionals.thank you.if possible do a vedios of pottasium Vs sodium in body how it's co related. Also hyperkalemia Vs hypokalemia
Thanks
can you guys PLEASE make more videos
Thank you.
I have been so freaking confused between Hyperkalemia and Hypokalemia and how they relate to Cardiac Arrest; correct me if I'm wrong, but I think it simplifies down to this: Hyperkalemia - the cell has difficulty contracting, Hypokalemia - the cell has difficulty relaxing
Great explanation. Great effort. All the best!!!!!
Thank you! the info was most helpful. please explain further more about the repolarization and why does the T wave raises respectively. thanks!
Have you meet any answer of Your question
I have the same qz?
"There appears to be a direct effect of elevated potassium on some of the potassium channels that increases their activity and speeds membrane repolarisation." You're welcome :))
I am brand new to understanding what hyperkalemia is. This was so confusing.
Very good. Thank you very much, from Brazil!
Very nicely explained ☺️.
So counter intuitive
amazing
if the potassium was high at the ECF; and since potassium is a positive ion, should the ICF would be more negative thus increasing threshold?
Threshold Potential does not move, but the RMP moves up closer to Threshold Potential if there is decrease in electric gradient: less K+ leaks from ICF to ECF, more K+ in ICF leads to decrease value (-90mV to -65mV) of RMP.
No it’s not about absolute values it’s about potential DIFFERENCE . RMP is the concentration gradient across the membrane. Suppose initially there were 100 k+ions inside and zero outside . The difference would be 100 making the rmp -100 mV . Now if 25 k+ ions move outside, only 75 remain inside making the difference 50 so rmp is now -50 mV which is closer to threshold potential. Hope this helps
@@bhartibajaj8730 but why do sodium channels decrease when threshold increases ?
What I don't understand is why hyperkalemia makes the membrane potential less negative? If you have more potassium ions in the extracellular fluid, doesn't that mean you have more positive charge outside? Wouldn't that make the membrane potential more negative?
exactly, this made me very confused.
if you got the answer can you please inform me?
i guess because -ve rmp is reached by efflux of k+ during repolariztion) (and this efflux depend on diffusion, its not active process, it depend on conc. gradient)
now as K+ can't leave (or to be more correct, less K+ is leaving cell because of the changed k gradient) cell wont reach the normal negativity (RMP), it will be less negative, this will make cell more excitable (its closer to firing thresold, less stimuli is required to reach firing level and causesing A.P (All na channels to be open)
but in severe hyperkalemia, a very little amount of K+ leave the cell, cell wont even reach the firing level, it will be higher than normal threshold level thus the inactivated sodium channel will stay in its inactivation state (inner inactivation gate still closed (remember that Na channels has 2 gates, one when activated causes depolarztion and other when activated close the channel and causes the absoulte r. peroid) ),,
in other word, it will stay in absoulte refractoy peroid -> less excistability (or even NEVER exctitable)
btw thats why K+ was used as execution injection, and thats why when K+ level reach 7mg/dl you should do dialysis right away, no time for insulin (althou the very rapid action of insulin)..
Let me try to make you understand
Hyper kalemia means inc levels of potassium in the ecf as we knis that potassium is 20 times more in icf comparred to ecf so just as thete is mkre potassium outside the potassium inside shall also increase to maintain a conc diff resultantly tye inside will become less negative and the membrane potential will bexome less negative as well or one can say partial state of depolarization it will never reach the rmp of compltetw its re polarization
Maybe its because of that inside of the cell, amount of potassium isnt changing. Instead of that we take more potassium from the outside. In the end we had more possitive ions in the ecf comparing with the first situation. That can be cause of less negativity of the membran potential.
Its because high conc of potassium outside will decrease the conc gradient across the membrane.. So less potassium will move out the cell.. Making the inside more positive or less negative
great job thanks so halpful and very clear explanation .more similar video please
Thanks for the video! But WHY does HyperK cause peaked T waves?
I have same query!
The T waves show you the electrical signal when the cardiac myocytes are repolarizing. I know that you need the sodium/potassium pump to work to restore concentration gradients... maybe that's an easier job when you're not fighting as high a concentration gradient so it goes up more quickly? That's probably wrong, but that's how I remember it...
How can ca+2 infusion helps in the treatment..?????
Do effect of hypercalcemia and hypercalcemia on heart
Why do you get peaked T wave in hyperkalemia? Even if the potassium efflux is slower
why is there less sodium channels available if the membrane potential Is too high?
But why do sodium channels decrease when threshold increases ?
Why does increasing the extracellular K+ concentration make the membrane potential having a more positive value? Thanks
The intracellular voltage becomes less negative in comparison to the more positive extracellular environment.
@@benstevens13 how? when the + ions are increased extracellulary, the intracellular space becomes even more negative! can somebody explain, please?
@@poljakovaandrea2223 you know when the gradient of an ion increases across membrane its tendency to move to side with lower conc. increases, so when overall potassium increases in serum more than normal of it would percolate in the cell making inside of membrane less negative. I hope it helps :)
@@travelfreak6901 Thanks! :)
how absolute value of resting membrane potential rises with decrease in potassium gradient around myocardial cell
Mam which is the first mineral and vitamin to be depleted in hair cells during stress causing sudden graying of hairs is it sodium chloride iron or copper.or calcium
welcome back
I had this pt who skipped her dialysis and came to ER for chest pain, she was bradycardic, she went unresponsive, her lab Potassium was 8.0 prior to hemodialysis. I don’t know if she survive, she left the room intubated, they took her for emergency hemodialysis.
How membrane potential becomes less negative when there is still the same amount of Kalium inside the cell and also same amaunt of negative charge. Should Hypercalemia outsuide of the cell contribute to positivity outside and thus increase potential difference from -90mv to maybe -120 mv and lead to hyperpolarization ?
Focus on the natural K+ leak channels. Less K+ leaks when hyperK in ECF (electric gradient is lessen). More K+ is retained in ICF that will move the RMP up closer to the AP threshold. Conversely, if hypoK+ occurs in ECF.
why hyperkalemia causes inactivation of sodium channels?
I have a hypotetical question, if I persons has CKF and also COPD, would that further increase the levels of K+??? I mean, the kidneys can't remove K+, the lungs keep building up CO2 in the blood which would leade to imbalance in PH since the cells would start exchanging K+ outside the cell and taking H+ in as a compensatory mechanism to reach back the normal levels of PH and correct the acidosis. In short, respiratory acidosis could worsen the increase of extracelular K+??? And also suppose that the patient takes Inhibitors of ACE, wouldn't that further spike K+ and maybe become a life threatening critical point to the patient's heart??
mechanism of action potential
Please what do you mean by magnitude of potassium gradient is increased across the cell membrane? Thanks in anticipation
Gradient = difference in potassium concentration between the inside and outside of the cell. Increased gradient = the difference is larger.
Why does K+ decrease when administering insulin? Doesn't insulin cause a shift of K+ into the cell, thus increasing total K+? Thanks.
Insulin moves K+ from outside the cells into cells, thus decreasing K+ OUTSIDE the cells. K+ outside the cells = K+ in the blood. It's the K+ in the blood that is important, not the total K+
ABOUT PROTEIN DISORDER
I have been getting changes in feeling like muscle tightening one moment and there is a looseness in muscles